



Eliminating Bias in Diabetes Care
Insight and Resources to Explore and Address Implicit Bias
Implicit Bias Defined
Understanding Its Impact in Diabetes Care
Research highlights the urgent need for practical education on implicit bias across all areas of health care. To ensure people living with diabetes receive equitable and appropriate treatment, health systems must equip providers with tailored education that directly addresses bias in clinical decision-making.
At ADCES, our work has explored how implicit bias shapes provider–patient interactions and influences access to medications, devices, and technologies. By fostering open dialogue, offering hands-on activities, and providing practical tools, we aim to raise awareness and give health care professionals actionable strategies to reduce bias in diabetes care. Here is a summary of one of these workshops hosted in August 2025. It includes participant experiences and strategies for mitigating bias.
What Is Implicit Bias?
Implicit bias refers to the deep-seated, often unconscious beliefs shaped by our upbringing, culture, and lived experiences. These beliefs influence how we perceive others, interpret their needs, and respond to them—sometimes in ways that unintentionally perpetuate inequities.
How Does It Manifest? Microaggressions
While implicit bias lives beneath the surface, microaggressions are its outward expression. They appear as subtle comments, actions, or behaviors that communicate bias, even when unintended. In health care, microaggressions may come across as indirect or unintentional discrimination against marginalized groups, such as racial or ethnic minorities, individuals with higher weight and those who are socioeconomically disadvantaged.
Why does it Matter in Diabetes Care?
In the context of diabetes care, biases and microaggressions can deeply affect clinical decisions, patient trust, and health outcomes. Both providers and patients may bring biases into the care relationship, creating complex dynamics that can hinder effective treatment. Addressing these issues is essential to ensure every person with diabetes has access to the best possible care and technology.
Perspectives
Impact on Diabetes Care Illuminated
Hear more about how implicit bias negatively affects diabetes care from health care professionals and people living with diabetes.

Veronica Brady, PhD, RN, FNP-BC, ACRN, BC-ADM, CDCES, FADCES

Christine Memering, MSN, RN, CDCES, BC-ADM, FADCES

Chelcie Rice
Examples
Ways that Implicit Bias Can Affect Care
Implicit bias can subtly influence many aspects of diabetes care — from screening and diagnosis to treatment decisions and patient communication. Recognizing these patterns creates an opportunity to strengthen equitable, person-centered care and improve health outcomes. Here are examples across different stages of care.
Assuming Type 2 Diabetes Based on Body Size
A clinician may unconsciously associate larger body size with Type 2 diabetes, which can delay evaluation for other forms such as Type 1 diabetes, LADA or MODY. It can also result in inappropriate medication prescriptions (e.g., oral agents when insulin is needed) and increased risk of complications such as DKA. Avoiding assumptions and conducting a full clinical evaluation supports timely and appropriate care.
Under-Screening in People Perceived as “Low-Risk”
Individuals who are thin, active or perceived as affluent may be screened less consistently if clinicians rely on stereotypes about who “looks like” they have diabetes. The potential Impact is higher glucose levels at diagnosis and increased risk of early complications. Consistent screening practices based on evidence-based guidelines — rather than assumptions — promote equity.
Less Intensive Treatment for Certain Groups
Research shows that Black, Hispanic and lower-income patients are sometimes less likely to be offered newer diabetes technologies (e.g., CGMs, insulin pumps). Assumptions about ability, cost, or sustained use may influence these decisions. The potential impact is unequal access to effective tool and widening disparities in outcomes. Equitable presentation of options and shared decision-making help reduce gaps.
Assumptions About Diabetes Management Challenges
When A1C levels are above target range, clinicians may assume lack of follow-through instead of exploring barriers such as medication cost, food insecurity, work schedules, cultural food traditions, or emotional stress. This can result in judgmental communication, reduced trust and missed problem-solving opportunities. Curiosity and partnership foster more sustainable solutions.
Differences in communication style
Implicit bias may influence tone, time spent, eye contact, and level of shared decision-making, resulting in the person feeling blamed or unheard and possibly disengaging in the treatment plan. Collaborative language strengthens trust.
Body size bias in counseling
People living with diabetes in larger bodies may receive repeated weight-focused messaging, even when other priorities need attention. Shame or additional stress may be a result, along with avoidance of care and delayed follow-up. Balanced, individualized counseling supports dignity and engagement.
Pain reports from marginalized communities may be underestimated, resulting in under-treatment of neuropathy and reduced quality of life. Validating symptoms and responding with empathy are essential.
Gestational diabetes results from complex hormonal and metabolic changes. Messaging that implies personal failure, particularly toward marginalized groups, can increase stress and reduce follow-up care. This can cause increased stress during pregnancy, reduced trust in health care team members and avoidance of postpartum diabetes screening. Supportive, nonjudgmental communication improves both short- and long-term outcomes.
Implicit bias does not operate in isolation. It can interact with structural systems in ways that compound disparities over time. Examples include:
- Referral patterns (Who is referred to endocrinology?)
- Access to diabetes education programs
- Assumptions about language proficiency
- Support with prior authorizations
- Access to diabetes technology
Small differences in these processes can accumulate, affecting long-term health outcomes. Recognizing these patterns creates an opportunity for healthcare teams to examine workflows, standardize equitable practices, and ensure that access to diabetes education, specialty care, and technology is guided by clinical need and personal preference — not assumptions.
Offering Diabetes Tech Consistently Across Patients
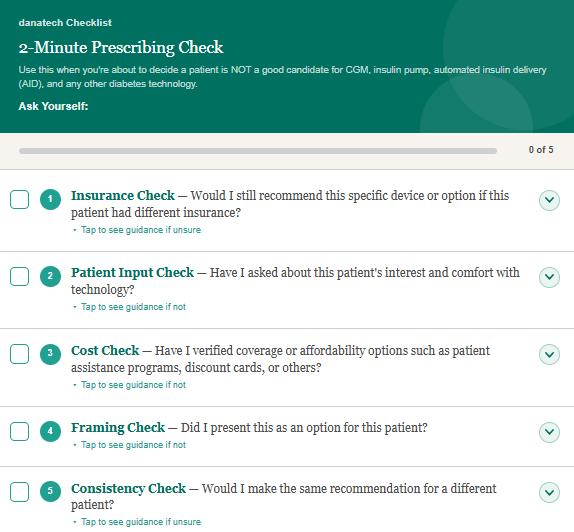
2-Minute Prescribing Check
Small variations in how diabetes technology is offered can lead to meaningful differences in access and outcomes. A tool, created by staff and the ADCES Diabetes Technology Committee, is designed to help clinicians pause, reflect and support more consistent and equitable decisions across their patient population. It offers a variety of checks covering: Insurance, Patient Input, Cost, Framing and Consistency.
Go to the 2-Minute Prescribing Check
The Data on Implicit Bias in Diabetes
Pediatric Endocrinologist and renowned researcher on bias, Ananta Addala, DO, MPH, offers an overview of the data on implicit bias in diabetes care, defines terms and share plenty of examples and solutions in this 17-minute presentation. "Seeing the Unseen: The Data on Implicit Bias in Diabetes" was presented at the ADCES Implicit Bias Summit in December 2024.
Watch the PresentationMore Research
Key Studies on Implicit Bias
The ADCES Research Committee conducted a review of recent research on the topic of Implicit Bias and members of the group provided brief commentary for each of the studies.
Stigma is extremely common in diabetes, with estimates of 60% of people with type 2 diabetes experiencing both diabetes stigma and weight stigma when interacting with their healthcare team. Trust in healthcare professionals, and perceived respect from healthcare professionals is an established predictor of perceived healthcare quality. One of the most common types of implicit bias is weight stigma which can be internalized or externalized. Many people with diabetes feel shameful, lonely, or hopeless about their diabetes and weight management. For people with diabetes, doctor’s appointments can feel like getting a report card or giving a big presentation if you have stage fright. To better understand the mechanisms involved in diabetes stigma, weight stigma, and healthcare interactions, 857 US adults with type 2 diabetes completed an online survey about their perceptions of their healthcare interactions, discrimination, and healthcare utilization. Participants who experienced negative interactions with their healthcare teams had higher rates of weight stigma and diabetes stigma. Importantly, delaying healthcare visits was more likely for participants with higher rates of weight stigma and diabetes stigma. These results provide support of the critical relationship between healthcare professionals and people with diabetes. Furthermore, these results illustrate a meaningful gap in healthcare education regarding reducing implicit bias to improve health outcomes and healthcare interactions. Of note, the survey questions did not specifically ask about interactions with diabetes care and education specialists.
Allyson Hughes, PhD
Citation
Sims, T.J., Kapoor, R., Chinthammit, C. et al. Relationship between Weight Bias Internalization, Diabetes Stigma, and Perceptions of Healthcare Interactions among People with Type 2 Diabetes. Diabetes Ther 16, 2025–2044 (2025).
A person’s activation describes their treatment-related knowledge, skills, confidence and behaviors that are associated with self-managing their condition effectively. Higher activation in diabetes is generally associated with greater diabetes self-management. In this observational, cross-sectional study, 857 adults with type 2 diabetes took a survey to assess their activation (IMPACT-D score) as well as surveys to assess weight and diabetes stigma and glycemic self-management. This study showed that among adults with type 2 diabetes, greater degrees of self-stigma were associated with lower degrees of participant activation and poorer glycemic self-management. Although exploratory, the findings suggest the need for increased efforts to support people experiencing weight and diabetes stigma, with the goal of increasing activation and improving glycemic self-management.
The findings from the BEAD-T1D Pilot Study were aimed at understanding perceived discrimination related to utilization of technologies vital to those with diabetes. The study explored the psychosocial state of minoritized families with type 1 diabetes with public insurance. Parents and guardians were recruited for either a survey, focus group, and/or parental advisory group. This pilot study was the first to take a deep dive into the relationship between psychosocial states, perceived discrimination, and diabetes management. Findings support the impact of discrimination from individuals and structural inequities. Although diabetes care and education specialists are not directly mentioned, the findings position them and other health care professionals to better support families in the adoption of important diabetes technologies. Technologies that are crucial to improving long-term health outcomes.
Leslie E. Kolb DrPH, MBA, RN
Citation:
Addala A, Medina Peñaranda R, Figg LE, Hanes S, Garfias Silva D, Ortega HI, Peña D, Shaw GM, Chamberlain LJ, Naranjo D, Raymond JK, Maahs DM, Hood KK. The Experience of Discrimination Impacts Technology Readiness and Psychosocial States of Minoritized Families Living With Type 1 Diabetes: Findings From the BEAD-T1D Pilot Study. Endocr Pract. 2025 Nov;31(11):1426-1434. doi: 10.1016/j.eprac.2025.06.023. Epub 2025 Jul 3. PMID: 40617391.
This article by Agarwal et al. (2020) provides an important scientific contribution by examining how a broad array of social determinants of health (SDOH) and disease-specific variables collectively influence glycemic outcomes in a national sample of emerging adults. This was a cross-sectional study leveraging the Type 1 Diabetes Exchange clinic network for participant recruitment. A major strength of this study lies in the thoughtful and intentional construction of its sample. The researchers recruited 300 emerging adults (ages 18-25) with T1D across six geographically diverse diabetes centers, ensuring near equal representation of non-Hispanic Black (n=97), Hispanic (n=103), and non-Hispanic White (n=100) participants. This level of demographic balance is rare in T1D research, where racial and ethnic minority groups are often severely underrepresented, especially among emerging adults. This intentional equal representation enhanced the authors’ ability to make balanced racial and ethnic comparisons. Furthermore, the sample was also economically and clinically diverse, with variation in insurance coverage (private, public, none), income level, diabetes technology use, and diabetes care setting.
The results of this study show substantial racial and ethnic disparities in meeting glycemic targets, diabetes technology use, psychosocial burden, and self-management. Importantly, non-Hispanic Black emerging adults consistently had the highest A1C levels, the lowest technology use, and the greatest levels of diabetes distress, even after accounting for socioeconomic status. However, Hispanic emerging adults had similar A1C levels to non-Hispanic White emerging adults, after accounting for socioeconomic status. Diabetes technology use, diabetes distress, and diabetes self-management contributed most to the disparity in A1C between non-Hispanic Black and non-Hispanic White emerging adults, out of all of the considerations captured. This illustrates that racial and ethnic differences in diabetes outcomes arise from social and contextual factors, and should not be considered inherent biological differences. Importantly, the authors of this article point out that in addition to cost, other factors such as personal and cultural preferences, clinician bias, literacy, and social support may drive disparities in diabetes technology use and diabetes outcomes.
Jorden Rieke, BSN, RN, CCRN and Quiana Howard MSN, RN-BC
Citation:
Shivani Agarwal, Lauren G Kanapka, Jennifer K Raymond, Ashby Walker, Andrea Gerard-Gonzalez, Davida Kruger, Maria J Redondo, Michael R Rickels, Viral N Shah, Ashley Butler, Jeffrey Gonzalez, Alandra S Verdejo, Robin L Gal, Steven Willi, Judith A Long, Racial-Ethnic Inequity in Young Adults With Type 1 Diabetes, The Journal of Clinical Endocrinology & Metabolism, Volume 105, Issue 8, August 2020, Pages e2960–e2969, https://doi.org/10.1210/clinem/dgaa236
Vela and colleagues conducted a systematic review to assess the efficacy of 25 studies with interventions designed to increase awareness of the harmful effects of bias. Most of the interventions increased the awareness of bias and interest in mitigating bias among participants. However, no study showed sustained decrease in implicit bias among health care providers and trainees.
Vela and colleagues suggest that the beneficial effects of provider level bias interventions are waned by structural biases in the work and learning environment of health care providers (e.g., racialized medicine) and structural inequalities outside the health care system (e.g., poverty, limited education, poor housing, healthy food scarcity). The authors present a conceptual model of implicit bias that illustrates how structural factors inside and outside of the HCS reinforce implicit bias. Work and learning environments with discriminatory practices send covert messaging to health care providers and trainees that reinforce biases. When caring for a patient with diabetes from a marginalized group, a provider’s bias may thwart communication resulting in suboptimal decision making. The patient, sensing the bias, distrusts the provider and does not disclose that he/she lacks the resources (e.g., money to purchase medications or healthy foods) to follow the provider’s instructions for self-care. This results in a poor health outcome that reinforces the provider’s bias. This vicious cycle promotes suboptimal health outcomes for marginalized groups, thus widening the health disparity gap. Provider level bias training should be accompanied by interventions that systematically change structures inside the healthcare system and increase awareness of structural inequalities within our society.
Eva Vivian, PharmD, PhD, MS, CDCES, BC-ADM, FADCES
Citation:
Vela MB, Erondu AI, Smith NA, Peek ME, Woodruff JN, Chin MH. Eliminating Explicit and Implicit Biases in Health Care: Evidence and Research Needs. Annu Rev Public Health. 2022 Apr 5;43:477-501. doi: 10.1146/annurev-publhealth-052620-103528.
Awareness of implicit bias continues to grow, though there is significant room for improvement. Implicit bias is, by nature, unconscious. Since it's not something that can be directly observed, it is difficult to address implicit bias without purposeful, intentional effort. But what are we to do about this problem?
This publication reviews practical ways we can recognize and address our unconscious biases in the context of diabetes care. The authors highlight how racial, ethnic, and obesity related biases can affect and shape clinical decisions and patient experiences. Not only do they raise awareness in this context, but the authors provide evidence-based recommendations to help reduce negative effects of implicit bias and improve overall care for people with diabetes. The authors provide guidance at both individual and systemic levels, and stakeholders across different roles can benefit. Readers will find that the review and implementation of available tools, recommendations, and data-collection strategies support providers, administrators, and anyone else involved in caring for people with diabetes.
Enrique Caballero, Nuha A. ElSayed, Sherita Hill Golden, Raveendhara R. Bannuru, Brigid Gregg; Implicit or Unconscious Bias in Diabetes Care. Clin Diabetes 15 April 2024; 42 (2): 308–313. https://doi.org/10.2337/cd23-0048
Research shows that physicians treating type 2 diabetes (T2D) consistently harbor moderate levels of bias and negative stereotypes toward their patients, despite generally feeling professionally prepared and confident in their ability to provide quality care (85%–86%). Among 205 surveyed physicians specializing in internal medicine or endocrinology, approximately one-third reported being repulsed by people with T2D, and substantial percentages endorsed negative stereotypes, viewing people with T2D as lazy (39%), lacking motivation (44%), and often “non-compliant” with treatment recommendations (44%). More than two-thirds believed individuals are personally responsible for developing T2D or that the condition is at least partially controllable. While weight stigma was slightly higher than diabetes stigma, the differences were small, suggesting the intersectionality of weight-based and diabetes-based stereotypes due to the frequent co-occurrence of obesity and T2D. These findings collectively demonstrate a pervasive level of stigma that requires urgent attention through targeted stigma reduction interventions for medical providers.
Researchers, Bennett and Puhl, used online questionnaires completed by physicians practicing in the U.S. who were predominantly male (72%) and White (79%), which limits generalizability to the broader physician population. Bias was significantly worse among younger physicians and those with fewer years in practice, and a higher percentage of people with T2D in a physician’s caseload was linked to greater lack of empathy and stronger beliefs about personal controllability. As this research was cross-sectional, future studies are needed to examine how physician bias impacts care quality, health outcomes, and healthcare avoidance. Meanwhile, integrating stigma-reduction strategies into medical education, continuing professional development, and clinical practice, such as using person-first language, addressing implicit bias in team training, and fostering compassionate communication, can help improve patient trust and outcomes.
Jennifer Rosselli, PharmD, BCACP, BC-ADM, CDCES
Citation:
Bennett BL, Puhl RM. Diabetes stigma and weight stigma among physicians treating type 2 diabetes: Overlapping patterns of bias. Diabetes Res Clin Pract. 2023 Aug;202:110827. doi: 10.1016/j.diabres.2023.110827. Epub 2023 Jul 13. PMID: 37451627.
Clinical decision-making is central to effective diabetes management, and a well-documented barrier to optimal decision-making is implicit bias. This innovative study was the first to investigate the influence of gender bias on clinical decision-making related specifically to type 2 diabetes. Participants were Dutch general practitioners. The study employed vignette-based scenarios (carefully constructed hypothetical clinical encounters that varied only by gender) depicting interactions between a person with type 2 diabetes and a healthcare professional. After reviewing the vignettes, participants rated the likelihood of various medical diagnoses, including the likelihood of a type 2 diabetes diagnosis. Participants also selected treatment recommendations and reported their confidence in the vignette character following their recommendations. Male general practitioners were more likely to diagnose male patients with type 2 diabetes, whereas female general practitioners were more likely to recommend motivational interviewing. Female participants were also more likely to diagnose with type 2 diabetes. Female vignette characters were much more likely to be referred to a dietician. Gender bias influenced not only diagnostic decisions but also treatment approaches. These results highlight the significant role of gender implicit bias in shaping the healthcare experiences and outcomes of people living with diabetes. Further, these findings provided clear evidence that general practitioners demonstrated gender-based implicit biases that affected their clinical decision making.
Allyson S. Hughes, PhD
Citation:
Skvortsova A, Meeuwis SH, Vos RC, Vos HMM, van Middendorp H, Veldhuijzen DS, Evers AWM. Implicit gender bias in the diagnosis and treatment of type 2 diabetes: A randomized online study. Diabet Med. 2023 Aug;40(8):e15087. doi: 10.1111/dme.15087. Epub 2023 Mar 23. PMID: 36919798.
This article demonstrated concrete evidence of bias in providers’ recommendations for technology in children and youth diagnosed with type 1 diabetes. What was surprising was that the bias was not race/ethnicity based but was insurance based. Thirty-nine providers from California, Colorado, Connecticut, District of Columbia, Massachusetts, North Carolina, Ohio and Texas participated. The majority (twenty-one) were from California, female and white. The group was comprised of physicians, nurse practitioners, and CDCESs, and eleven (28.2%) had a diagnosis of type 1 diabetes themselves. Thirty-three out of thirty-nine providers demonstrated bias against recommending technology for patients on public health insurance. This bias was not affected by age but was affected by years in practice. The longer someone was in practice the more likely they were to show bias in not recommending continuous glucose monitors for patients on public insurance; it was the second factor in order of importance for many providers.
When it came to recommending insulin pumps there was less bias, it was the fourth factor out of seven ranked. In both cases race/ethnicity came last. It was encouraging to see that family preference was the first thing considered by providers for both CGM and insulin pumps and that in both cases race/ethnicity came last. The authors theorized that providers, having practiced for longer, had previously had trouble getting diabetes technology covered through public insurance. So, a potential solution would be to provide updates on how to get technology covered through public insurance as well as updates on American Diabetes Association (ADA) guidance changes. The ADA now recommends diabetes technology for all patients with type 1 diabetes based on shared decision-making and patient/family preference. This is heartening news since a bias rooted in practical insurance and knowledge barriers can be more easily fixed. Some limitations of this research intervention are the small sample size (thirty-nine) and the lack of racial and gender diversity (predominantly white and female).
Liseli Mulala, RPh, MPH, PhD, CDCES, BCMTMS
Citation:
Addala A, Hanes S, Naranjo D, Maahs DM, Hood KK. Provider Implicit Bias Impacts Pediatric Type 1 Diabetes Technology Recommendations in the United States: Findings from The Gatekeeper Study. Journal of Diabetes Science and Technology. 2021;15(5):1027-1033. doi:10.1177/19322968211006476
Recent advances like automated insulin pumps and continuous glucose monitors have reduced the daily burden of diabetes management and lowered risks such as hypoglycemia and diabetic ketoacidosis. However, access to these technologies is not equal—race, ethnicity, and socioeconomic status strongly influence who receives education and uses these devices. To address these disparities, Singh and colleagues (2025) examined what factors drive technology use and how provider practices affect recommendations. A large chart review was conducted to see if socioeconomic factors like insurance type explained differences in diabetes technology use. The study also surveyed children with diabetes and their caregivers during clinic visits to learn their views on the benefits and challenges of using devices. Finally, clinic providers were surveyed about their prescribing practices for diabetes technology.
Black and Hispanic youth were far less likely to use insulin pumps or continuous glucose monitors than White youth, even when insurance and HbA1c were similar. These families often learned about technology later, while most White families were introduced at diagnosis. Caregivers with limited English perceived more barriers to technology use. Overall, Black and Hispanic families had positive attitudes toward these devices, showing that low use is not due to lack of interest. Providers often based decisions on subjective factors like family stability and health literacy instead of clear clinical criteria; this suggests access to technology depends more on provider perceptions than medical need. This study underscores the need for increased provider awareness of personal bias when providing diabetes care and education; additionally, standardized clinical guidelines are essential to ensure all families receive timely education and equal access to diabetes technology. Clear, consistent communication between providers and patients—paired with structured clinical practices—can reduce barriers and improve outcomes for everyone managing diabetes.
Synneva Hagen-Lillevik, PhD, MS, RD
Note: The content of is solely the responsibility of the author and does not necessarily represent the official views of the National Institutes of Health.
Citation:
Singh, P., Garcia, A., Grishman, E. K., Naranjo, D., Hynan, L. S., Lau, M., White, P., & Gupta, O. T. (2025). Disparities in diabetes technology utilization in youth with diabetes. BMJ Open Diabetes Research & Care, 13(6), e005067. https://doi.org/10.1136/bmjdrc-2025-005067
Experienced stigma is the stigma that people are aware of and can talk about; whereas, internalized stigma is what they take in and becomes part of who they are, how they think about themselves, and how they feel about and manage their health. Internalized stigma can include self-devaluation and applying weight-related stereotypes to oneself. Self-devaluation is a form of personal blame for one’s body weight. Internalized stigma and self-stigma are sometimes used interchangeably.
This survey study examined experienced and internalized stigma and the impact they have on HbA1c in adults with type 2 diabetes. The authors studied survey responses from 857 English-speaking adults with type 2 diabetes and found that 47.8% had experienced weight stigma. Those who reported HbA1c > 4-8% experienced the least weight stigma and had the lowest mean BMI. Those who reported HbA1c > 8.01 – 20% experienced the most weight stigma and had the highest mean BMI.
Internalized weight bias, weight self-stigma, and diabetes stigma were significantly higher in those who reported HbA1c > 8.01 – 20% than those who reported HbA1c > 4-8%.
Across the board, Hispanic participants reported the greatest weight stigma and diabetes stigma, including both internalized and experienced stigma. White participants were consistently next in line with Black participants reporting the least amount of stigma in all categories. There were no significant differences between White and Hispanic participants for weight bias, and there were no significant differences among the three groups for diabetes stigma; however, Hispanic and White participants reported significantly more weight bias than Black participants.
Participants who reported higher HbA1c levels experienced greater weight stigma and diabetes stigma. One-third of participants did not report HbA1c (in this study they were most likely to be Hispanic) and reported similarly greater levels of weight stigma and diabetes stigma. This finding is alarming because it is impossible to know if those people did not know their HbA1c, did not know what HbA1c is, or were afraid to report it. The authors mentioned that HbA1c may be seen by people with type 2 diabetes as a “measure of performance.”
Eighty-eight percent of respondents reported their HbA1c within 4-8%, which does not align with national statistics and could represent response bias or a skewed sample. The fact that Hispanic and White participants reported the highest levels of bias and stigma could be related to cultural differences among the three groups, which leaves many unanswered questions, requiring further research on this important topic.
Jane Dickinson, RN, PhD, CDCES, FADCES, FAAN
Citation:
Sims, T.J., Chinthammit, C., Constantine, M.L. et al. Examining the Relationship Between Weight Stigma, Diabetes Stigma, and HbA1c in Adults with Type 2 Diabetes. Diabetes Ther 16, 2137–2156 (2025). https://doi.org/10.1007/s13300-025-01795-8
Uncovering and Understanding Your Hidden Biases
Project Implicit, a nonprofit organization and international collaborative of researchers interested in implicit social cognition developed this well-known and respected test. Often referred to as the Harvard Implicit Association Test, it explores your attitudes and beliefs about a variety of topics and indicates whether or not there may be an automatic preference or implicit bias present. The results can help us to reflect and understand our actions, decisions and attitudes that can be related to discriminatory practices and ideologies.
Learn more and take the test
Thank You To Our Sponsors
Thank you to our sponsors, whose commitment helps advance equity-focused education for the diabetes care and education community.
Supporting Sponsor: Lilly
Partner Sponsors: Abbott, Dexcom, Medtronic